

Ron Canonigo, PT, DPT, prepares a patient for the parallel bars. “Simply asking the patient to stand up and walk down the hall for you might not be enough to determine the patient’s overall function,” Canonigo says. Photography by Rogena Silverman
I help sick people walk again—at least, that’s how my 7-year-old son describes my career as a physical therapist. If only it were that straightforward.
As a therapist at Northridge Hospital Medical Center, Northridge, Calif, I have the opportunity of working with patients following stroke or traumatic brain injury at all levels of the continuum of care—from early on in the hospital’s intensive/critical care units and cardiovascular/cardiopulmonary units, through transition in the medical-surgical units and acute rehabilitation unit, through outpatient therapy, as well as the hospital’s comprehensive brain injury day treatment program. At every stage of a patient’s rehabilitation, functional mobility—including gait and balance—is typically assessed.
PHYSICAL ASSESSMENT
At the time of the initial assessment, and before every treatment session, I must decide if a patient is ready to begin physical therapy intervention. This is determined by measuring blood pressure, monitoring the individual’s heart rate, and checking lab values (if available). It should also be a priority to monitor the patient about how they are feeling before, during, and after the assessment or treatment session, as well as constantly keep track of their signs and symptoms. At times, I believe that this part of the assessment is not emphasized enough, and patients often have additional medical conditions to address.
My approach to assessments is quite simple, really. Before I look at someone run, I look at that person walk. Before they run, I want to see if the person can hop, first on two feet maybe holding onto parallel bars, then on one foot. Before I see how a person walks, I look at how they perform a sit-to-stand, and then standing posture. When a patient is in a hospital bed, before I look at sitting balance, I want to see how they move their extremities, neck, and trunk. However, before I observe any physical movement, it is important to assess the patient’s alertness and ability to follow instructions. At every level of the continuum of care, including acute, subacute, home health, and outpatient care, knowledge of these fundamental tasks I believe can help keep the clinician mindful of areas that might easily be overlooked. Simply asking the patient to stand up and walk down the hall for you might not be enough to determine the patient’s overall function.

The author and a client work on high level balance on an unstable surface while performing trunk rotation holding a weighted ball.
In the American Physical Therapy Association’s Guide to Physical Therapy Practice, there are a variety of standardized tests that are used to objectively measure a patient’s overall functional mobility and balance. The 6-Minute Walk Test, Berg Balance Scale, Clinical Test of Sensory Interaction for Balance (CTSIB), Functional Independence Measure (FIM), Stroke Rehabilitation Assessment of Movement (STREAM) Measure, and Tinetti Performance-Oriented Mobility Assessment all demonstrate various levels of validity and reliability. Although not listed in the guide, a couple of other tests are worth mentioning: the Dynamic Gait Index (DGI) and the Balance Evaluation Systems Test (BESTest). The DGI rates performance on eight different gait tasks: gait on even surfaces, changing speeds, gait with horizontal and vertical head turns, gait with pivot turns, stepping over and around obstacles, and stairs. The BESTest is a 27-item measurement tool that encompasses many of the above-mentioned tests, and includes an assessment on sitting balance, standing balance, response to perturbations, modified-CTSIB, in addition to gait tasks, and the timed “get up and go.”
There is a variety of information available on the 4-Item DGI and the 14-item mini-BESTest. There are pros and cons for each of the tests. From patient to patient, severity of impairments can vary widely; some tests are maybe too easy and you experience a ceiling effect, while other tests are maybe too difficult and you experience a floor effect. The right test, or tests, should at least incorporate a combination of a motor control assessment, timed balance in sitting and/or standing, and a timed locomotor distance, whether in a wheelchair or ambulation with or without an assistive device. In addition to objective measures, a gait analysis should also be included. As Perry and Burnfield highlight in Gait Analysis: Normal and Pathological Function, second edition, the Classification of Stroke Disability, as described by Mulroy, says, “Understanding pathological gait in the population with head injury and identifying the areas of impairment which compromise stride length symmetry and hinder gait velocity, should guide the clinician toward the most effective treatment. By simply measuring gait distance and grading the level of assistance needed without addressing the areas of impairment, will likely result in accomplishing the goal of ambulating further but with significant compensatory patterns.” What is more important: quantity or quality?
EQUIPMENT PRESCRIPTION

The balance and gait programs Canonigo designs can include a partial body weight support gait therapy device to help facilitate standing balance or ambulation.
If an assistive device is needed, determining the appropriate one is generally not decided at the time of discharge, but likely a process throughout the continuum of the rehabilitation program. There are numerous possibilities: power or manual wheelchair, the traditional rollator, front-wheel walkers with or without bilateral forearm supports, wide-base or narrow-base quad canes, or single point canes. Although not generally considered to be in the same category as assistive devices, using a sit-to-stand lift device or partial body weight support gait therapy device to “assist” with facilitation for standing balance and/or ambulation, respectively, should also be considered. Although it might take some patient education on my part when recommending one piece of equipment versus another—ultimately, I leave it up to the patient to decide what equipment is most appropriate so they are also invested in the decision-making process.
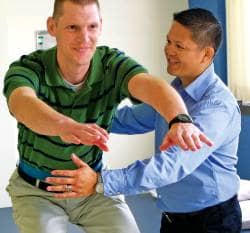
Canonigo uses what he describes as a “simple” approach to assessments. “Before they run, I want to see if the person can hop. Before I see how a person walks, I look at how they perform a sit-to-stand, then a standing posture,” Canonigo explains.
For patients affected with severe, unilateral upper extremity weakness, it might be appropriate to use an arm sling, or a sling that acts as a positioning device for the flaccid upper extremity, to reduce excessive subluxation of the involved shoulder when sitting or standing. An arm sling may also improve the patient’s trunk posture and assist with progressing ambulation. I recommend that the arm sling be worn primarily during activities out of bed. The sling should probably not be worn throughout the entire day, or when in bed, to avoid issues such as muscle and/or joint contractures, skin breakdown in the antecubital fossa, pressure sore on the olecranon, or impaired circulation. For individuals with lower extremity weakness, an ankle foot orthosis (AFO) would be the likely recommendation, or possibly even a functional electrical stimulation device. A variety of options are available depending on the amount of support needed for the given task, many manufactured with material durable enough to withstand running with them. Discussing these options with an orthotist, as well as consideration of the patient’s comfort and preference, will likely result in the best outcome. In ideal circumstances, we should all hope that all of our patients will become functionally independent and will not have to rely on any assistive device.
Ultimately, the ability of the clinician to appropriately assess patients with brain injury, from either stroke or traumatic injury, is not always that straightforward. Severity of impairments can vary widely from patient to patient. Using the appropriate assessment tool in order to objectively measure the patient’s progress would generally be considered best practice. Selecting the appropriate assistive device should include informed patient preference. It may not seem like much to the general public but for those patients who may require my expertise—I help them walk, and sometimes even run, again.
Ron Canonigo, PT, DPT, is the primary physical therapist at Northridge Hospital Medical Center Brain Injury Day Program, Northridge, Calif, as well as an APTA-credentialed clinical instructor and a member of both the Acute Care and Oncology Sections of the APTA. For further information, contact the .


