

Corporal Todd Nicely, who sustained quadrilateral amputations, is undergoing metabolic analysis as part of a research protocol.
Walking is a critical part of our daily lives that is often taken for granted until it is disrupted by trauma, disease, or painful conditions involving our muscles, bones, or nervous system. When evaluating patients who have sustained traumatic brain injuries (TBIs), limb loss, or other neurologic or orthopedic injuries, the initial physical therapy evaluation often states that the patient’s goal is to walk. Service members recovering from battle-related injuries are no exception, though they may go a step further and state that running and return to duty are their goals.
Due to the mechanism of combat-related injuries, more often than not, there are confounding orthopedic, neurologic, and/or psychological trauma. Many of the patients have sustained fractures or amputations in addition to varying degrees of TBI, all of which may be further confounded by post-traumatic stress disorder. This makes rehabilitation even more of a challenge.
The term “evidence-based medicine” was introduced in the 1990s1,2 and has been defined by Sackett et al1,3 as “the conscientious, explicit, and judicious use of the current best evidence in making decisions about the care of individual patients.” It is a systematic process whereby pertinent objective data is gathered, synthesized, and applied to individual cases to optimize patient care. At Walter Reed Army Medical Center (WRAMC), we use computerized gait analysis to provide objective details of the joint movements, associated forces, and patterns of muscle activity to aid clinical decision-making. In the civilian sector, use of such technology has been validated as a means of providing an objective measure of a patient’s walking pattern.4 It is widely reimbursed for pre- and post-operative management in pediatric neurologic disorders. At WRAMC, 3-D gait analysis is used to lend insight into causes of gait deviations, optimal treatment plans including orthotic and prosthetic prescription or alignment, effectiveness of interventions (eg, physical therapy technique or modality, pharmacology, bracing, prosthetic components, and surgery), and patient progress over time.
The biomechanics lab, where the 3-D gait analysis data is collected, is located within the Military Advanced Training Center (MATC) Center for Performance and Clinical Research (CPCR). The area is a 49- x 35-foot space that accommodates a 49-foot (15 m) walkway, which allows for collection of data at steady state walking or running.
DATA AND EQUIPMENT
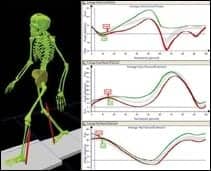
3-D kinematics are collected by 23 high-speed cameras simultaneously recording the movement of the head, trunk, and extremities as a person walks via tracking of retro-reflective markers. The views are merged to construct a 3-D model that is then used to calculate joint motion in each of the three planes. The data can be represented in graphic form to show the dynamic range of motion (ROM) during gait.
Temporal-spatial parameters are also derived from marker data. Events, or phases of gait, are identified during post-processing in order to report velocity, cadence, percent time spent in stance phase, step length, and step width.
Kinetic data is derived from six forceplates located in the floor of the lab that measure force in three planes representing (1) braking and propulsion, (2) generation and absorption, and (3) medial-lateral shear. From this data, the moments and powers can be calculated about the lower extremity joints.
The instrumented treadmill has two embedded forceplates and can incline or decline 15°. This is often used when collecting sustained walking or running data for metabolic analysis.
Metabolic data includes oxygen uptake, energy expenditure, and heart rate. Oxygen uptake and heart rate are collected on a breath by breath cycle; changes from resting to steady state activity and recovery are documented.
In electromyography (EMG), surface electrodes are applied to the skin overlying the muscles to be studied. The phasic muscle activity data that is collected is synchronized with the kinematic data so it can be analyzed according to the different phases of gait.
EVALUATION PROCESS
The evaluation process starts with an appropriate referral from a clinical care provider. This begins with a question, eg, “Does the current prosthetic alignment or programming contribute to an optimal gait pattern?” “What intervention facilitates a more efficient gait pattern, an ankle foot orthotic or a foot drop stimulator (functional electric stimulation unit)?” or “Does the current dosage of antispasticity medication positively impact function?” Of course, validated measures like the 6 minute walk test can be conducted to enhance the clinical picture but often fail to quantify quality of movement. Some questions cannot be objectively and comprehensively answered by observational gait analysis. The primary limitation of this method is that the human eye cannot observe, process, and interpret complex multisegmental movements simultaneously. Computerized gait analysis can bridge the gap.
Referrals can be initiated at any phase of the rehab process that the primary care provider deems necessary. A clinical history is obtained from the patient, referral source, and electronic notes. A screening physical exam is performed to include assessment of ROM, strength, muscle tone, motor control, sensation, and balance on the day of testing. If sEMG is indicated, surface electrodes will be placed over the muscles to be studied. If metabolic data is being collected, the appropriate preparation is made (eg, donning heart rate monitor, metabolic mask, and securing transmitter).
The patient is then prepared for the computerized gait analysis. About 60 retro-reflective markers are applied to specific landmarks on the patient’s body. These markers are tracked by the motion capture cameras and create a stick figure on our monitor; the presence of real-time feedback ensures that we are collecting usable data. Typically, subjects are then asked to walk at their normal pace. They are observed and simultaneously videotaped from the front, back, and right and left sides. Since one’s self-selected velocity is most efficient, if the patients are able to walk at a faster, forced velocity, that data is collected as well. By walking at a speed faster than self-selected, deviations that are masked by slow velocities can be magnified. This provides valuable real-world application. The entire collection process takes between 1 and 2 hours, depending on how many conditions are tested.
INTERPRETATION OF RESULTS
Several computers are used to collect the 3-D and metabolic data, perform temporal-spatial, kinematic, and kinetic calculations, and process the information into a format for interpretation. This dynamic information, combined with physical examination, observational analysis, and medical history, contributes to a complete picture of an individual’s walking pattern. Postprocessing can take 1 to 4 hours; reports can be generated in an hour. Report reviews typically range from 30 to 60 minutes and include the patient and caregiver, evaluating PT, referring clinician, and other available care providers who deal directly with aspects of patient care related to ambulation.
A computer program reflects images and graphs of the collected 3-D and metabolic data for the therapist’s review.
In analyzing pathological gait, normal function is the model against which the abnormal gait is compared. Deviations from the normal pattern define the functional compensation needing attention. Patient data is compared with control data of uninjured service members collected in our lab.
Review of temporal-spatial data may reveal asymmetries in step length and stance time, the source of which may be explained by the physical evaluation. For example, if a patient has a right hip flexion contracture or spasticity, they may take a shorter step on their contralateral side. Typically, if patients display a wide base of support (increased step width), it may be indicative of instability. Of course, it is not always clear-cut. Investigating the physical evaluation as a means to explain a time-distance deviation will require substantiation of that theory. Further support for the proposed theory can be obtained by looking at kinematics.
In the above stated example of a patient with a unilateral hip flexion contracture, it would seem obvious to look at the sagittal hip graph. The graph may show decreased peak hip extension on one side compared to the other and/or controls. If it does not, the investigation continues. Joints above and below are evaluated to identify where the compensation is taking place. In the case of hip flexion contractures, one would most likely anticipate an anterior pelvic tilt. All planes and all lower extremity joints, pelvis, and trunk are thoroughly reviewed to further develop the problem list. Once the temporal-spatial and kinematic data are reviewed, kinetics are assessed to see if they corroborate the theory.
When evaluating kinetics, it is important to keep in mind that they are velocity-dependent measures, ie, the faster the velocity, the higher the kinetic parameters. Vertical ground reaction force is normalized to body weight. It gives an indication of whether a patient is favoring one side or the other. It also provides insight into rate of loading and unloading. Power generation and absorption are other key parameters of interest because they give objective measures of function of prosthetic components, AFOs, or the lower extremity joints themselves. Moments further define what muscles must be active, based on knowledge of biomechanics and the current objective picture painted by the kinematics and temporal-spatial components.
TREATMENT PLANNING
Once a problem list is generated, it is then prioritized. If the top three or four problems are resolved, they should, in turn, resolve the other related problems. In the case of a patient with a unilateral amputation and ipsilateral hip flexion contracture, PT interventions will not release the contracture. The focus can shift to prosthetic care. The prosthetist may be able to sufficiently modify the socket alignment or components to allow for a more symmetric gait pattern. There will still be compensations, but general function and possibly energy cost and quality of life may be improved. The patient can be reevaluated or consider other (surgical) interventions with their care providers. With all members looking at objective data from their discipline-specific vantage point, the patient is actively engaged in representing their own goals and concerns with the medical professionals charged with their care. This is the case for all patients, regardless of diagnosis, age, rank, or specific rehabilitation goals. Our mission is to provide the best and most efficient care to those who have selflessly served our country.
CONCLUSION
We are very fortunate to have the technological resources available to objectively impact efficiency of patient care. Our experience has been that 3-D gait analysis can benefit patients of varied diagnoses. We also acknowledge that gait labs are not widely available, nor are they a widely reimbursable benefit outside of pediatrics. It is our belief that outcomes for an array of patient populations can be expedited by eliminating the trial and error method; this is cost-effective in the long run. To validate our method of utilization of this technology, we also are conducting research on various military patient populations. It is our hope that dissemination of the objective findings will justify the use of 3-D gait analysis for appropriate patient populations in the civilian sector.
Please read “The Walking Wounded Warrior: The Assessment and Treatment Progression of Wounded Service Members with Gait and Balance Dysfunction,” an online exclusive.
Barri L. Schnall, MPT, has been managing the Center for Performance and Clinical Research at Walter Reed Army Medical Center, Washington, DC, since 2001. For more information, contact .


