
The rehabilitation patient’s dress rehearsal for discharge.

Graduation Day! 3-2-Free is the culmination of inpatient rehabilitation, and the team celebrates with a graduation ceremony as the patient prepares to discharge.
Traumatic spinal cord injuries (SCIs) affect more than 12,000 individuals in the United States each year.1 Comprehensive rehabilitation for persons who sustain an SCI requires a team approach to reach established patient goals (CARF).2 During rehabilitation, goals are often set to ameliorate impairments noted in body function/structure, activity, and participation based on the International Classification of Functioning, Disability, and Health (ICF) model adopted by the World Health Organization (WHO), and progress toward activity-based goal attainment is commonly measured by the Functional Independence Measure (FIM).3 This is the required outcome measure for rehabilitation facilities serving Medicare patients to manage reimbursement and to benchmark other facilities via the Uniform Data System.3 To ensure data entry is accurate, rehabilitation administrators may choose to audit this data for accuracy of assessment and scoring. This is the case at Shepherd Center in Atlanta, where more than 300 patients affected by SCI are treated each year.
The FIM requires that staff document the amount of actual assistance a patient needs versus what the patient is potentially capable of performing, ie, burden of care versus abilities.3 During routine audits, it was noted some patients were not meeting expected FIM outcomes. However, according to team communication and other documentation, it appeared the patient—in fact—did have the capacity to perform these skills. This conflicting information revealed a need to improve the accuracy of reporting. Staff focus groups and patient and caregiver interviews were conducted to better understand the causes behind the variations that emerged in the reporting. The outcome of those efforts revealed that the following had contributed to inaccuracies in reporting:
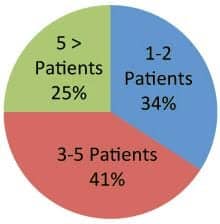
Table 1. Staff exposure to 3-2-Free at time of the survey
- Staff time constraints did not allow patients to demonstrate their abilities to perform all aspects of their care.
- Patients reported they were unclear that they were expected to perform all of their care at their maximum capacity as discharge approached.
- It was challenging to have the patients combine the skills required in their daily routine.
- Patients and caregivers alike expressed great anxiety about their ability to manage care in the home environment. This anxiety routinely escalated as the discharge dates approached.
- Staff reported they were unsure of the patients’ true abilities and expectations.
Based on information gathered from these discussions and interviews, a team of clinicians developed a more structured program to better prepare patients for discharge. The program was designed to more clearly define expectations so that all stakeholders in the rehab process would be aware of the functional potential for each patient. The program was named 3–2–Free; it begins 3 days before discharge and functions as a “dress rehearsal” for the patient. The program had three objectives: 1) improve overall goal attainment; 2) conduct self-report surveys among patients and caregivers to guage the preparedness prior to discharge; 3) allow staff to express better understanding of a patient’s true abilities to perform activities of daily living, transfers and mobility skills, and verbalization ability for those skills for which they are dependent.
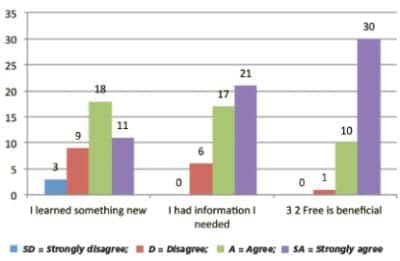
Table 2. Summary of Staff Survey Questions
PROCESS IMPLEMENTATION
To create the 3-2-Free program, an implementation group was assembled that included all disciplines that would be involved in the program: case managers; counselors; nurses; occupational, physical, and recreation therapists; and speech and language pathologists. This group met for five, 1-hour sessions to define the mission of the program, establish the role of each discipline, and develop tools to communicate the patient’s goals. Through this collaborative effort, 3-2-Free provided a framework around which patients could increase their own confidence in the ability to perform, and/or direct, their activities of daily living and functional mobility to the greatest potential during the final 3 days of inpatient rehabilitation.
Given the large number of staff members who interact with each patient daily, the implementation group decided that communicating the mission, structure, and importance of the program among stakeholders would be imperative to the program’s success. To support this communication, staff, patient, and caregiver education tools were developed. Patients were scheduled for a 15-minute educational class to learn more about the expectations for 3-2-Free prior to its initiation. Expectations for the program also were added to a mandatory caregiver orientation class that occurs at the time of admission. (See Box 1, page 19, for implementation tools.) A large goal sheet was developed outlining all personal care needs, functional transfers, and community outings that should occur within the last 3 days of rehabilitation. On the goal sheet, the appropriate therapist notes the level of assistance the patient requires for each task based on their functional potential. Next, one team member discusses the individualized expectations with each patient. The goal sheet is posted in the patient’s room as a monitoring tool, so that the nursing staff is informed of the patient’s performance potential. Nursing is then able to communicate whether the patient successfully meets each goal. In addition to performing functional tasks independently, the patient is expected to plan for and request scheduled medications. Prior to the start of 3-2-Free, a medication administration log is created by the nurse and the patient, and posted as a second monitoring tool.
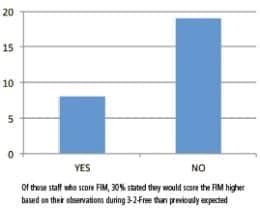
Table 3. FIM scoring results
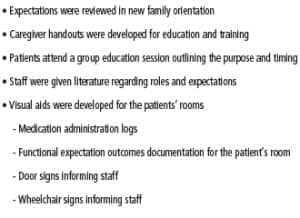
Box 1. Process implementation resources
As part of the efforts to strengthen communication and understanding about 3-2-Free among staff, visible notifications to inform all staff members (including nights/weekends) of each patient’s participation in the program were developed. A flag is carried in the patient’s wheelchair backpack and a large sign is hung on the door of the patient’s room (Figure 1, page 19), announcing that the patient is in 3-2-Free. Additionally, weekend therapy and nursing coverage notes indicate if the patient is currently in the program, enhancing continuity and engagement for all clinicians involved in that patient’s care. Finally, graduation T-shirts were designed to capture this milestone in the patient’s rehabilitation process (see photo at top).
MEASURING OUTCOMES

Figure 1. Door sign for staff and family notifications
To help determine the effectiveness of 3-2-Free, staff surveys were conducted for those clinicians who had patients participating in the program (n=44). The overall objective was to obtain the following information: 1) staff’s perceived understanding of the program; 2) availability and usability of developed tools; 3) for those staff who score the FIM (n=27), the frequency the FIM score reflected a change due to observation made during the 3-2-Free program; and 4) staff’s realization a patient could perform a task or direct their own overall care during the 3-2-Free time period, which they otherwise would not have known. Table 1 (above) describes the number of patients specific health care providers had treated who had participated in the program at the time of the survey. Results indicated staff perceived they had the tools they needed (87%). The survey also revealed that the patient could perform or direct their own care as a result of the 3-2-Free program (72%), and that the patient benefited from participation (98%) (Table 2, above). For those who routinely score the FIM (n=27), 30% reported they scored the patient’s outcome higher on the FIM due to 3-2-Free observations. Table 3 (above) summarizes these findings. Several comments made during the survey process are shared in Box 2 (below).
Box 2. Sample anecdotal comments from the staff survey
Survey results also uncovered several areas in which improvement was needed. These areas included team communication, caregiver’s expectation, and ease of documentation—specifically, medication administration. Staff reported that caregivers expressed confusion about whether they were supposed to perform the care or if the focus was the patient only. Staff also expressed confusion early in the implementation process and required further education to clarify that the focus should be on the patient performing the skills or directing care, and not on training for the family or caregiver. While caregiver training may take place while 3-2-Free is in progress, the primary focus of the program must be the patient and how well that individual models behaviors that will be essential at time of discharge.
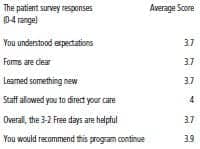
Box 3. Patient survey results (N=14)
During the process development and the pilot program, 15 patients were surveyed at completion of their programs. The subject’s responses to the 3 2 Free program were overwhelmingly positive, and reported in Box 3 (page 20). One key point of interest was whether a patient learned they could perform a skill or direct their own care as a result of participating in the 3-2-Free program. It was noted that 13 patients out of 14 patients who answered the survey agreed or strongly agreed they had achieved this objective. Furthermore, 100% of patients who completed the survey reported they agreed or strongly agreed the program should become a part of routine care. Favorable reactions also were apparent in remarks made by patients and recorded on the surveys, such as, “3-2-Free helped me know what I can do for myself,” and “I felt like I had more freedom and independence.” Anecdotally, there was one patient who participated in the program who was dependent in all aspects of her care, and had to verbally direct her personal care, transfers, and daily activities. Prior to 3-2-Free, she reported she was terrified to discharge because she had to go temporarily to another facility. She was concerned that staff at a different location may not be as familiar with her care needs as the staff at Shepherd Center. By the end of the 3 days, she successfully met her goals and remarked that she was no longer afraid to discharge because she knew she was capable of directing all of her care. While outcome tools, such as the FIM, do not measure these aspects of participation, they are vital to the patient’s overall well-being.
Overall, 3-2-Free was developed with minimal time requirements from staff and with simple organizational processes and communication tool implementation. Staff and patients agree that the program enhances rehabilitation outcomes and improves patient confidence and demonstrated abilities prior to discharge.
Shari McDowell, PT, is Director of Spinal Cord Injury Services at Shepherd Center, Atlanta. McDowell has practiced as a PT for 26 years with 20 years being at Shepherd Center treating people with spinal cord injuries. Her areas of expertise include SCI rehabilitation, critical and acute care following SCI, education, and administration.
Ginger J. Perritt, MS, OTR/L, is an occupational therapist at the Shepherd Center, Atlanta. Perritt has practiced occupational therapy for more than 7 years, with 6 years treating primarily spinal cord-injured clients at Shepherd Center. Her areas of expertise include inpatient SCI rehabilitation, dual SCI and ABI diagnosis, women’s issues associated with SCI, and bladder management.
Both McDowell and Perritt participated in research associated with the 5-year SCIRehab Study. For more information, contact .
REFERENCES
- Spinal Cord Injury Facts and Figures at a Glance. National Spinal Cord Injury Statistical Center, Birmingham, Ala. www.nscisc.uab.edu; February 2012.
- Medical Rehabilitation Standards Manual. Commission on Accreditation of Rehabilitation Facilities, 2011.
- Inpatient Rehabilitation Facilities Patient Assessment Instrument. UB Foundation Activities Inc, 2001-2004.



