

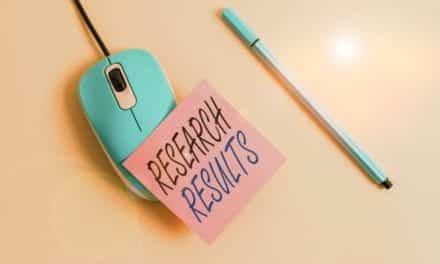
Male pediatric client uses a walker to work on his mobility goals. His core muscles are strong, and with bracing, he is able to ambulate.
by Meredith Budai, PT, DPT, ATP/SMS, CRND, and Erin Neuland, PT, DPT
Pediatric physical and occupational therapists have the unique challenge of providing opportunities to children with physical disabilities. These children may not otherwise be able to achieve age-appropriate milestones due to physical disability. The goal is to provide means for early exploration and participation for children with disabilities at the same age as their non-disabled peers. Therapy goals should be comprehensive and encompass many aspects of the child’s life, including interacting with their environment and their peers.
Mobility Milestones
Exploration and mobility can be provided through the use of supported standers, gait trainers, and wheelchairs. Upright mobility, achieved with a stander, provides the opportunity for children to interact with others and participate in age-appropriate play, which is integral for proper development. Mobility is vital for development of the child in many realms, including cognitive development, social development, and communication skills.
Among children there is a direct correlation between physical mobility and the achievement of certain developmental milestones. During typical development, children begin rolling at around 3 to 4 months. It is then that a child will begin to interact with the environment. Similarly, crawling begins at approximately 9 months of age and ambulation between 12 and 18 months. Standing permits a child to have significantly greater access to the environment. On the other hand, children with limited standing opportunities to interact with the environment often experience developmental delay and cognitive impairment. Immobility is also a major contributing factor in strength impairments and can lead to serious health consequences. For example, these health consequences can lead to a shift toward greater fat mass, which causes cardiovascular impairments and increases the risk of further secondary complications throughout the life span.
Preparation for Standing
The American Academy of Pediatrics recommends a minimum of 20 to 30 minutes of exercise three times a week. Among children with functional limitation, standers, gait trainers, and walkers can assist with increasing mobility and, therefore, exercise. Standers have been shown to promote cardiovascular strengthening, prevent contractures, improve range of motion, decrease spasticity, improve bone health, improve organ function, and improve overall arousal levels in individuals. Equipment, such as a stander, gait trainer, or walker, can prevent further injury and deterioration in the health of children. Developmental stage and functional ability of the child will determine the appropriate mobility equipment for the individual. There are a variety of different types of standers available to the pediatric community.
Prior to standing, the clinician should determine whether the child is ready for a weight-bearing program. Clearance should be obtained from the physician indicating that a child is safe to stand and presents without orthopedic limitations, including, but not limited to, increased risk of fracture or weight-bearing restrictions. The child should have sufficient hip, knee, and ankle range of motion to minimize stress placed on the joints. If the child does not have sufficient range of motion, physical therapy services should emphasize stretching and, if necessary, tone management.
Careful consideration should also be given to the type of stander that a child should use, as some standers may be able to accommodate for range of motion deficiencies. In addition to having sufficient range of motion, a child should be able to tolerate standing at 80 degrees to 90 degrees without signs or symptoms of orthostatic hypotension. Signs and symptoms may include feelings of light-headedness or nausea, fatigue, or blurry vision. If a child is unable to tolerate upright standing, that child should start out using a tilt table during physical or occupational therapy. A tilt table allows a child to gradually transition from supine to standing, allowing the body time to acclimate to the change in positioning. Once the child tolerates standing for
30 minutes at 80 to 90 degrees, they are ready to be evaluated for the appropriate stander or gait trainer.
Standing Technologies
Standers can be static, active, or dynamic. Each type of stander provides varying levels of support for lower-extremity positioning, trunk positioning, and upper-extremity support. Static standers simply allow the user to bear weight on their lower extremities with no active movement and are typically the most supportive of standers. Active standers allow for gliding motions that can increase cardiovascular output in the individual. Dynamic standers are typically mobile and can be propelled by the user. These commonly provide the least amount of support when compared to other types of standers.
Another dynamic option is a wheelchair standing device. These combine power- or manual-wheeled mobility and standing through the use of one device, thereby eliminating the need to transfer from one device to another. In some of these wheelchairs, the user is able to propel the chair in the standing position. These are typically power wheelchairs, and they include safety features that limit the speed while in the standing position.
Standers can also be categorized by positioning features and level of support. For instance, children who are classified as physically dependent and lack motor control from the neck and below often require a supine stander. This means that the child is placed on their backs and secured with straps and positioning devices before safely transitioning to standing. An example of this is a tilt table. As was previously described, children who are intolerant to upright may also benefit from this type of device due to the gradual transition to standing.
Alternatively, some children have improved tolerance when transitioning to standing from a seated position. These types of devices are known as sit-to-stand standers. These require that the child has slightly more motor control than a supine stander. These standers still offer a variety of positioning options as required.
Finally, a prone stander requires that a child has strong back extensors as the support is provided primarily on the anterior surface of the child’s body. Prone standers are typically mobile, as they allow freedom of movement in the trunk and arms for propulsion. How much support an individual needs, how functional the upper body is, and their medical stability will help guide the decision of which type of standing device one would choose.

An 8-year-old female pediatric client uses a prone, mobile stander. The large wheels provide mobility without hurting her arms.
Gait Trainers and Walkers
If a child has volitional control in the lower extremities, specifically in the hip flexors and extensors, a gait trainer may be appropriate. A child who benefits from a gait trainer typically requires more support than a standard walker can provide. Gait trainers tend to be bulkier and more stable than walkers, and can provide partial weight-bearing. A gait trainer capitalizes on volitional control and allows for reciprocal stepping movements of the legs while providing support of the pelvis, since these children typically cannot stand unsupported and may require additional support at the trunk or extremities. Gait trainers provide many support options, including seats with increased trunk and pelvic control that can provide varying amounts of off-weighting to make ambulation easier for the child.
A walker can be used by a child who requires only the arms for balance and support. It does not provide any additional pelvic or trunk support. When choosing a gait trainer or a walker, it is important to try various options and sizes to determine the appropriate fit. Many considerations should be made regarding the child’s functional ability, amount of support needed throughout the body, spasticity, and hand function. As with standing, children should be medically cleared for weight-bearing and upright positioning by their doctor prior to utilizing a gait trainer or walker. Utilization of gait trainers and walkers is imperative in children with motor deficiencies to reduce the risk of motor delays.

The support provided by a prone stander is on the front surface of the body.
Upward and Onward
From the time infants begin rolling, they are developing cognitively by exploring their environment. Children with physical disabilities may require the assistance of supportive devices to allow for similar interaction with their environments. These devices provide children with opportunities they would otherwise be unable to experience. Standers, gait trainers, and walkers allow for continued exploration, cognitive development, strengthening, and decreased secondary complications due to immobility. RM
Meredith Budai, PT, DPT, ATP/SMS, CRND, is a clinical specialist at the International Center for Spinal Cord Injury at Kennedy Krieger Institute in Baltimore. She received her bachelor of science and bachelor of health sciences in 2006 and her Doctorate of Physical Therapy in 2008 from Duquesne University in Pittsburgh. Budai has been a certified assistive technology professional since 2011, a certified seating and mobility specialist since 2015, and is on the board of examiners for rare neurological disorders. She has presented nationally on activity-based rehabilitation principles and their application in pediatrics and with seating and positioning recommendations. Her clinical interests are pediatrics, functional electrical stimulation, casting and orthotics, and seating and mobility. She is experienced in wheelchair prescription, aquatic therapy, and land therapy for children and adults with neuromuscular diagnoses.
Erin Neuland, PT, DPT, has been a physical therapist since 2011 working in an adult inpatient rehabilitation center prior to coming to the International Center for Spinal Cord Injury (ICSCI) at Kennedy Krieger Institute in October 2012. She received her Doctorate of Physical Therapy from Old Dominion University in Norfolk, Va, and her Bachelor of Arts degree in Mathematics from Hood College in Frederick, Md. She has a particular interest in aquatic therapy, casting, gait training, and early upright mobility. For more information, contact [email protected].



Interesting post, I am going to spend more hours learning about this subject.