
 |
At the Assistive Technology Center, Spaulding Rehabilitation Hospital, Boston, occupational therapist Peggy Dellea, MS, OT/L, is stationed on the front lines of neurological rehabilitation. Representing a good portion of Dellea’s patient load are individuals who suffer from the progressive, debilitating effects of amyotrophic lateral sclerosis (ALS). Dellea works to keep this contingent of formerly vital men and women slightly ahead of the physical deterioration that chases after them by outfitting them with assistive technology designed to preserve their function.
Neurogenic pathologies encompass many disorders such as stroke, traumatic brain injury, multiple sclerosis, and Parkinson’s disease. All are capable of comprehensively disabling the human body, yet it is ALS that stands apart from the others, notorious for the speed with which it separates patient from function. A typical case runs its course in 2 to 5 years from the point of diagnosis, and the diagnosis is always terminal.
“With ALS, there is no cure,” Dellea says. “Treatment tends to focus on symptom management and optimizing functional independence and quality of life.”
Absent of a medical solution, the disease spurs a kind of necessary kinship between patients and the technology that has been designed to keep them employed longer at their jobs and engaged with family and community.
Retooling the environment for patients who sooner or later will come to rely on assistive technology must be considered from a long-term perspective, according to Dellea, who focuses on computer adaptation and building user expertise to forge a connective seam between patients and their high-tech aids. The link she establishes will be used to coax out and capitalize on what-ever function remains with a patient throughout the progression of their disease.
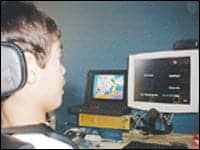 |
| Jackson Fischler, a 9-year-old boy with cerebral palsy, uses a system controlled by his eye movement, that enables him to compose electronic messages, play video games, and run assistive technology to participate in school. At left, he controls a program on his laptop with such a system. |
The technology-based assistive devices Dellea might use can occasionally be glimpsed on medically themed television programming such as ER or Discovery Channel. Dellea points out those depictions often can leave individuals in the early stages of ALS with a distorted expectation of how the technology will perform.
“Patients see Stephen Hawking on television and come in and say, ‘I want what he has.’ What they don’t see is the part about him building the sentence before he says it,” Dellea says. The magic of the television cutting room, she explains, makes the communications system used by the famed physicist—who suffers from ALS—appear deceptively fast.
The learning curve and cost of assistive technologies available to individuals who have degenerative neurological conditions can span a wide range. Some computer operating systems available to the general public provide built-in accessibility features that are often overlooked, yet can effectively assist with communication and allow users to execute voice-activated tasks. By educating patients about how to use such features, Dellea says she is able to provide a valuable resource for no more than the cost of the software.
Higher up on the cost continuum are systems controlled only by the user’s eye movement, which allow individuals to compose electronic messages, play video games, and run popular computer software. Such systems can synthesize speech for nonverbal users, such as Hawking, as well as provide environmental control over lights, appliances, and televisions.
“When patients get to the point where the eyes are the only thing over which they have good control, that becomes their access point,” Dellea says.
As a patient’s access point moves through the degenerative process, functional ability shifts as well, a fact that leads Dellea to underscore the importance of developing patients’ expertise with an assistive technology before they become dependent on it.
 |
| Mike Toennis, who has ALS, “speaks” with his wife, Karen, and Dixon Cleveland using a system controlled by his eye movements. Cleveland is a vice president of development for the system manufacturer. |
“We consider a patient might make only one big purchase. At first, it’s to help them type, then maybe they’re using it with a head mouse, and later, as the disease progresses, they switch to the eye-controlled system.
“The whole system must be considered in terms of how it will be used from diagnosis to end stage,” Dellea says.
Ultrasophisticated assistive technologies are not always as difficult to use as might be expected, yet Dellea cautions that not all high-end systems are without a challenge. Certain voice recognition packages, for example, can be made to appear almost effortless to command under the control of experienced users. In reality, such systems can take up to 12 hours of training before new users develop operational proficiency.
“In the 11 years I’ve been working with these systems, I’ve seen only two people who were able to buy the software, put it on their computer, and run with it,” Dellea says.
The use of assistive technology is not restricted to the critically disabled, and no technology has made an impact felt so profoundly among the broader population of people who have neurologic impairment as the personal computer, Dellea says. The devices, rare in American households when she began her career in 1993, have made what the veteran therapist considers the most significant contribution in nearly a generation toward the goal of extending the functional abilities of those who struggle with neurological disability.
“People come in with their Facebook and MySpace, and it’s their lifeline to communicating with family and friends. They can keep up with what’s happening; they can shop online for groceries and gifts, pay bills—it’s opened up opportunities and uses that simply were not possible before,” Dellea says.
FINDING BALANCE AMONG THE “LOST PATIENTS”
Individuals who suffer balance and vestibular disorders are not always consigned to the downward spiral experienced by ALS patients. However, says Lisa Brown, PT, rehabilitation programs for individuals affected by balance and vestibular conditions lie far beyond the boundaries of a one-size-fits-all solution.
“I love the challenge of the neurological patients,” Brown says. “You can line up five stroke patients and have them present to you with very different levels of deficit, and all of them may have very different goals in mind for their outcomes,” she observes.
Brown, a practicing therapist for 14 years, has spent the last 7 years at Spaulding Rehabilitation, Framingham, Mass, treating individuals who have balance and vestibular disorders. She focuses on maintaining her patients’ balance and visual reflexes as well as building strength and proprioception in their lower extremities. Brown says her patients, who represent an often disregarded corner of neurological rehabilitation, seem to benefit most when pushed to do task-specific training and exercise.
“If you want to improve walking speed, you would work on walking speed and can do treadmill training with patients that can help carry over,” Brown says. “You can work on transfer with sit-to-stand exercises, not only promoting a better functional carryover but also tapping into neuroplasticity changes we’re seeing.”
Gaze stabilization exercises, Brown says, also are useful in recovering balance function. “Visual exercises, for example,” Brown explains, “where you ask a patient to focus on a word [helps them with the ability] to move their head while they’re keeping that word in focus.”
Successful outcomes, in Brown’s estimation, are often anchored by keeping patients as independent as possible inside their homes, whether an individual has suffered a stroke or spinal cord injury. Training patients specifically to the activities they most want to do ensures that essential rehabilitation activity is carried over outside the clinic. A patient’s own support system, too, Brown points out, can make a dramatic difference in shaping an outcome.
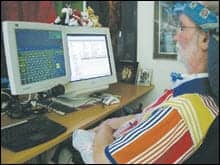 |
| ALS patient Paul Stevens, retired Navy program manager and CFO of the National Speleological Society, works to extend his functional capacities by using assistive technologies. He uses a system controlled by his eye movement to operate a variety of standard commercial computer applications. |
“It’s great for family members to see the functional things a patient can accomplish, and encourage them to carry over those functional tasks at home—versus when you have an acute injury, and family tend to want to be overprotective and ‘do’ for the patient,” Brown says.
Brown characterizes vestibular patients as a “lost group,” which she says is particularly interesting to treat.
“I felt like I was helping this group of patients who didn’t seem to have a lot of resources for them,” she says. As a patient population, individuals who suffer from balance and vestibular disorders are often simply given medication and told their symptoms will disappear on their own, according to Brown. Vestibular suppressing medications, she explains, only delay the recovery process.
Watershed changes driven by a decade of research and clinical work are changing how the therapy community thinks about the recovery process—and particularly about neuroplasticity. The touchstone of the new thinking is a collection of data that suggests many types of rehabilitation for a variety of conditions can be effective throughout a period much longer than previously thought possible.
“When I got out of school 14 years ago, we were treating patients and saying, ‘OK, we have a few months after their injury and then that’s it. That’s the best recovery we’re going to get.’
For more information on neurological rehabilitation, search our free online archives.
“Now it’s being shown that if you are able to retrain the patient appropriately or fairly aggressively, then even 5 or 10 years after the injury, they can make some fairly significant gains,” Brown says.
“We also know now that the more we can push our patients and the longer they’re able to tolerate a treatment, the better the outcomes,” says Brown. “The research that’s coming out is so promising, and it’s just starting to get translated into the clinic, which makes it an incredible time for any therapist—just out of school or with 30 years of experience—to be in this kind of field.”
Frank Long is the associate editor of Rehab Management.
Without A Voice
Spasmodic dysphonia leaves bodies to function in silence.
Human speech is physiologically enmeshed in nerve and muscle activity that stretches from the ears to the abdomen. Spasmodic dysphonia is an uncommon, frequently misdiagnosed neurological impairment that causes vocal cords to spasm and tighten but remain apart—devastating the normal speech process. The disorder causes extreme disability in interpersonal communications, yet leaves an individual otherwise physiologically able to conduct the activities of daily life.
“Most people who have spasmodic dysphonia end up having to quit their job or leave their careers,” Catherine Moore, BA, MA, says. “They can whisper, yell, or sing, but people who have the disorder can no longer speak normally.
“It shatters the patient’s life as they’ve known it,” Moore says.
Spasmodic dysphonia is one of the more uncommon communicative disorders Moore treats at her Brea, Calif, practice. The symptoms are marked by labored, choked speech that has lost much of its volume. Because physicians can often mistake spasmodic dysphonia for early symptoms of cancer or Parkinson’s disease—or consider the symptoms psychogenic in nature—individuals can struggle with the condition for years before receiving a correct diagnosis and proper treatment.
“Patients are told they have severe laryngitis or gastroesophageal reflux disorder, or maybe just a voice tremor,” Moore says, adding that the condition does not cause pain but is known to produce sensations such as a throat tickle, tightness in the neck, breathlessness, or fatigue. The disorder can also push sufferers to overcompensate for their impaired speech by using clavicular breathing rather than the more correct diaphragmatic breathing.
While struggling to cope with a condition they do not fully understand, some individuals inadvertently stumble onto a correct diagnosis in the process of seeking help for problems that arise from other focal disorders, such as torticollis or blepharospasm, conditions that often lead to an appointment with a neurologist.
Susi Pensel was a veteran marketing professional who battled the symptoms of spasmodic dysphonia for 15 years before receiving a proper diagnosis. Pensel never considered she was in the throes of a serious neurological disorder and, instead, dismissed the quivering and tightness in her throat as the by-products of career stress and marital issues. The stresses eventually subsided, but the restriction in her voice grew steadily worse.
“It was exhausting trying to push to speak,” Pensel says, recalling the escalating difficulty of verbally expressing ideas to coworkers or making important presentations to clients. After a series of referrals and an examination by a physician who specialized in the disorder, Pensel was handed a correct diagnosis but waited nearly 2 years before moving forward for treatment.
After conducting her own research, Pensel eventually chose a treatment plan that included therapeutic injections of botulinum toxin A (BTX).
Injecting BTX locally into the vocal cord muscles diminishes muscle spasms by blocking the nerves’ ability to stimulate vocal muscles. Spasmodic dysphonia occurs in an adductor form, abductor form, and mixed form, with each variation demanding a slightly different treatment approach. Using BTX to treat the abductor form, for example, is often less effective because of the difficulty involved in making injections to muscles that lie behind the larynx.
According to Moore, an injection of BTX by itself can improve the client’s voice for 4 to 20 weeks. A combination of BTX injection and voice therapy, Moore adds, typically provides optimal results for a client.
Pensel underwent a series of five BTX injections in a 2-year period and says she experienced short-term benefits from the treatment.
“I’m an athlete, and I was running and inline skating at the time I was getting the injections. The BTX stopped the dramatic spasms, but I couldn’t get enough air in to walk up stairs, let alone continue running.”
Pensel abandoned the injections in favor of speech therapy.
Designing an effective therapy program, Moore says, demands a highly individualized approach that includes a variety of vocal techniques and takes into consideration the outcomes of interventions the client has already tried.
“A technique that works for an adductor client may not work for an abductor client, so we look at what is effective for a specific condition and build on it,” Moore says.
After conducting an initial discussion to address specific problems and outcome objectives, Moore moves the client into an assessment period that is tape recorded so that changes in voice quality that occur while different techniques are practiced can be quickly identified. Clients experiment with techniques such as chant talk, moving the voice to the forward mask, or using yawning and sighing to minimize tension. Through this process, techniques that match a client’s needs begin to emerge.
Techniques that work during Moore’s voice therapy sessions become the client’s homework for the week.
“I practiced diligently,” Pensel says, recalling the therapy assignments she received as one of Moore’s clients. “Speech therapy was more effective for me than the BTX injections. I learned to breathe properly again and to stop engaging my shoulders and upper body when trying to speak.
“I’d walk around the house saying, ‘Hello, hello,’ trying to change my pitch upward, trying to bring my voice to my facial mask. I’d sometimes use a British accent.
“All of it helped,” Pensel says.
In an effort to restore voice function to their clients, speech therapists can look to assistive technologies, just as physical therapists do in treating patients in a clinical setting who are neurologically involved.
Computer software packages aid therapists by creating a visual representation of a client’s speech characteristics such as pitch, loudness, duration, and spectra patterning. Moore says the technology helps clients improve speech function by allowing them to “see” changes in their voice as visual depictions.
Inside her home, Pensel is assisted by an amplified telephone that boosts the volume of her voice, which can sound faint to untrained ears. She has also taken advantage of a portable, two-piece voice amplifier—similar to devices used by tour guides—to boost her voice in social settings. Pensel says for her, however, the device was not effective.
“I’m very animated, and the voice amplifier was cumbersome,” Pensel says. “I moved around a lot and the device didn’t move with me.”
Moore says individuals who suffer with the condition over the long term experience a gamut of emotions in adjusting to a condition that has no cure. Moore says her clients sometimes withdraw socially and experience feelings of hopelessness and isolation. Yet, she says, they can also exhibit tremendous resilience and through their struggle with the disorder build sympathy, compassion, and an appreciation of the positives in their lives.
“I am very clear on this,” Pensel says, reflecting on her lifetime diagnosis.
“I’m extremely fit and I feel terrific, even though I sound terrible. I have a friend who used to be an athlete and who now has multiple sclerosis and can move only one arm.
“I’m grateful for what I don’t have,” Pensel says.
—Frank Long



